

A wheelchair (W/C) is a seat with wheels, mainly used for people with functional impairment or other walking difficulties. Through wheelchair training, the mobility of disabled people and people with walking difficulties can be greatly improved, and their ability to carry out daily activities and participate in social activities can be improved. However, all of these are based on a major premise: the configuration of a suitable wheelchair.
A suitable wheelchair can prevent patients from consuming too much physical energy, improve mobility, reduce dependence on family members, and facilitate comprehensive recovery. Otherwise, it will cause skin damage, pressure sores, edema of both lower limbs, spinal deformity, risk of falling, muscle pain and contracture, etc. to patients.

1. Applicable objects of wheelchairs
① Severe reduction in walking function: such as amputation, fracture, paralysis and pain;
② No walking according to doctor's advice;
③ Using a wheelchair to travel can increase daily activities, enhance cardiopulmonary function, and improve quality of life;
④ People with limb disabilities;
⑤ Elderly people.
2. Classification of wheelchairs
According to the different damaged parts and residual functions, wheelchairs are divided into ordinary wheelchairs, electric wheelchairs and special wheelchairs. Special wheelchairs are divided into standing wheelchairs, lying wheelchairs, single-side drive wheelchairs, electric wheelchairs and competitive wheelchairs according to different needs.
3. Precautions when choosing a wheelchair
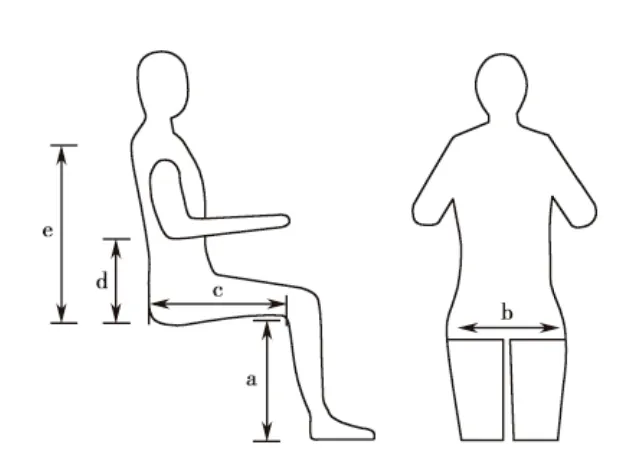
Figure: Wheelchair parameter measurement diagram a: seat height; b: seat width; c: seat length; d: armrest height; e: backrest height
a Seat height
Measure the distance from the heel (or heel) to the dimple when sitting, and add 4cm. When placing the footrest, the board surface should be at least 5cm off the ground. If the seat is too high, the wheelchair cannot be placed next to the table; if the seat is too low, the ischial bone bears too much weight.
b Seat width
Measure the distance between the two buttocks or the two thighs when sitting, and add 5cm, that is, there is a 2.5cm gap on each side after sitting. If the seat is too narrow, it is difficult to get on and off the wheelchair, and the buttocks and thigh tissues are compressed; if the seat is too wide, it is not easy to sit steadily, it is inconvenient to operate the wheelchair, the upper limbs are easily fatigued, and it is also difficult to enter and exit the door.
c Seat length
Measure the horizontal distance from the buttocks to the gastrocnemius muscle of the calf when sitting down, and subtract 6.5cm from the measurement result. If the seat is too short, the weight will mainly fall on the ischium, and the local area is prone to excessive pressure; if the seat is too long, it will compress the popliteal area, affect local blood circulation, and easily irritate the skin in this area. For patients with extremely short thighs or hip and knee flexion contracture, it is better to use a short seat.
d Armrest height
When sitting down, the upper arm is vertical and the forearm is placed flat on the armrest. Measure the height from the chair surface to the lower edge of the forearm and add 2.5cm. The appropriate armrest height helps to maintain correct body posture and balance, and can place the upper limbs in a comfortable position. If the armrest is too high, the upper arm is forced to lift up and is prone to fatigue. If the armrest is too low, the upper body needs to lean forward to maintain balance, which is not only prone to fatigue, but may also affect breathing.
e Backrest height
The higher the backrest, the more stable it is, and the lower the backrest, the greater the range of motion of the upper body and upper limbs. The so-called low backrest is to measure the distance from the seat to the armpit (one or both arms stretched forward), and subtract 10cm from this result. High backrest: measure the actual height from the seat to the shoulder or the back of the head.
Seat cushion
For comfort and to prevent pressure sores, a seat cushion should be placed on the seat. Foam rubber (5~10cm thick) or gel cushion can be used. To prevent the seat from sinking, a 0.6cm thick plywood can be placed under the seat cushion.
Other auxiliary parts of wheelchair
Designed to meet the needs of special patients, such as increasing the friction surface of the handle, extending the brake, shockproof device, anti-slip device, armrest installed on the armrest, and wheelchair table for patients to eat and write.


4. Different needs for wheelchairs for different diseases and injuries
① For hemiplegic patients, patients who can maintain sitting balance when unsupervised and unprotected can choose a standard wheelchair with a low seat, and the footrest and legrest can be detachable so that the healthy leg can fully touch the ground and the wheelchair can be controlled with the healthy upper and lower limbs. For patients with poor balance or cognitive impairment, it is advisable to choose a wheelchair pushed by others, and those who need help from others to transfer should choose a detachable armrest.
② For patients with quadriplegia, patients with C4 (C4, the fourth segment of the cervical spinal cord) and above can choose a pneumatic or chin-controlled electric wheelchair or a wheelchair pushed by others. Patients with injuries below C5 (C5, the fifth segment of the cervical spinal cord) can rely on the power of upper limb flexion to operate the horizontal handle, so a high-back wheelchair controlled by the forearm can be selected. It should be noted that patients with orthostatic hypotension should choose a tiltable high-back wheelchair, install a headrest, and use a removable footrest with adjustable knee angle.
③ The needs of paraplegic patients for wheelchairs are basically the same, and the specifications of the seats are determined by the measurement method in the previous article. Generally, short step-type armrests are selected, and caster locks are installed. Those with ankle spasms or clonus need to add ankle straps and heel rings. Solid tires can be used when the road conditions in the living environment are good.
④ For patients with lower limb amputation, especially bilateral thigh amputation, the center of gravity of the body has changed greatly. Generally, the axle should be moved back and anti-dumping rods should be installed to prevent the user from tipping backward. If equipped with prosthesis, leg and foot rests should also be installed.
Post time: Jul-15-2024